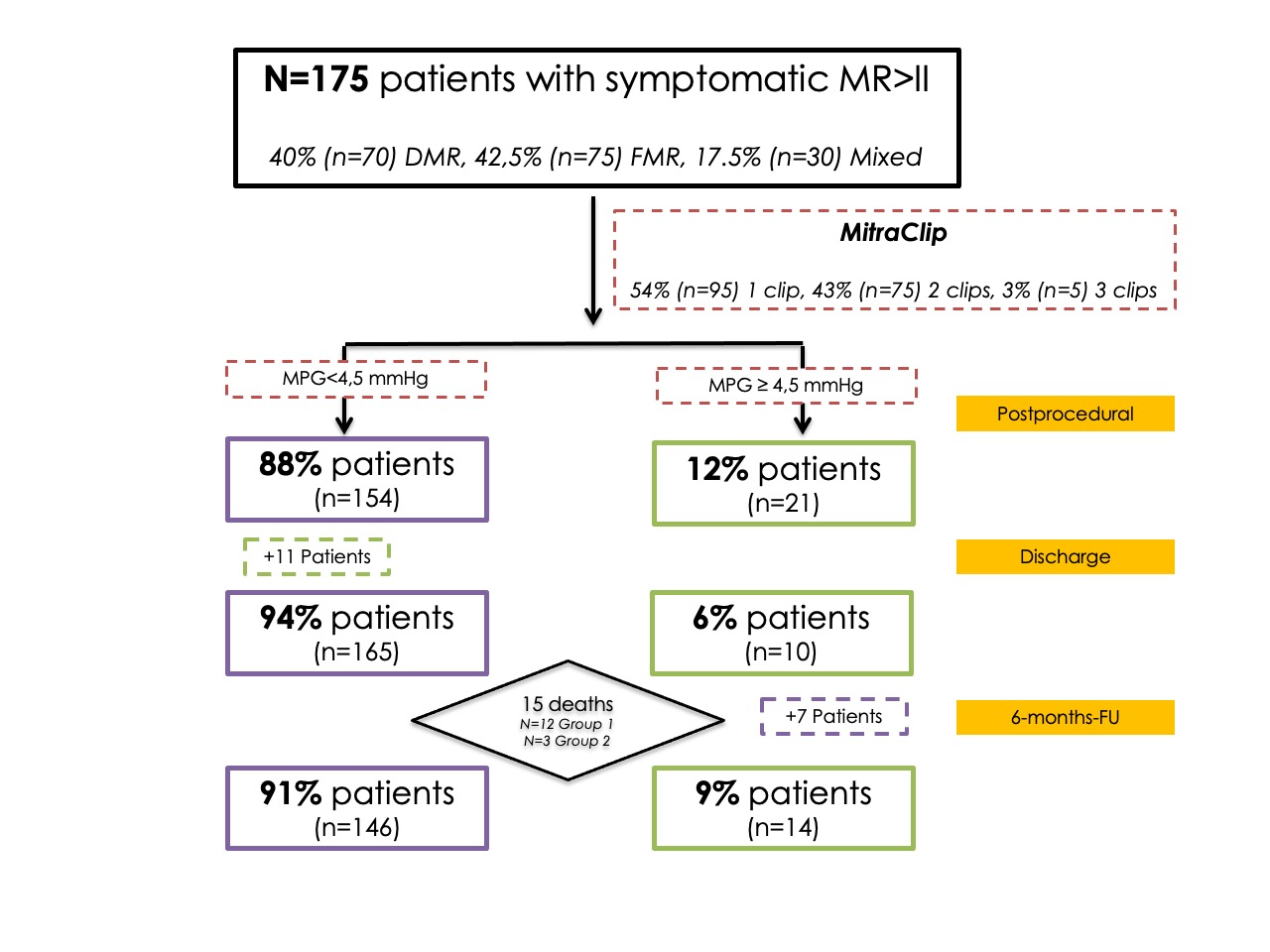
Background: The impact of the increased mitral gradient (MG) on outcomes is ambiguous. Therefore, we aimed to evaluate a) periinterventional dynamics of MG, b) the impact of intraprocedural MG on clinical outcomes, and c) predictors for unfavourable MG values after MitraClip. Methods: We prospectively included patients undergoing MitraClip. All patients underwent echocardiography at baseline, intraprocedurally, at discharge, and after six months. 12-month survival was reassessed. Results: 175 patients (age 81.2±8.2 years, 61.2% male) with severe mitral regurgitation (MR) were included. We divided our cohort into two groups with a threshold of intraprocedural MG of 4.5 mmHg, which was determined by the multivariate analysis for the prediction of 12-month mortality (<4.5 mmHg: Group 1, 4.5 mmHg: Group 2). Intraprocedural MG 4.5 mmHg was found to be the strongest independent predictor for 12-month mortality (HR: 2.33, p=0.03, OR: 1.70, p=0.05) and ≥3.9 mmHg was associated with adverse functional outcomes (OR: 1.96, p=0.04). The baseline leaflet-to-annulus index (>1.1) was found to be the strongest independent predictor (OR: 9.74, p=0.001) for unfavourable intraprocedural MG, followed by the number of implanted clips (p=0.01), MG at baseline (p=0.02) and central clip implantation (p=0.05). Conclusion: MG shows time-varying and condition-depended dynamics periinterventionally. Patients with persistent increased (≥4.5 mmHg) MG at discharge showed the worst functional outcomes and the highest 12-month mortality, followed by patients with an intra-hospital decrease in MG to values below 4.5 mmHg. Pre-interventional echocardiographic and procedural parameters can predict unfavourable postprocedural MG.