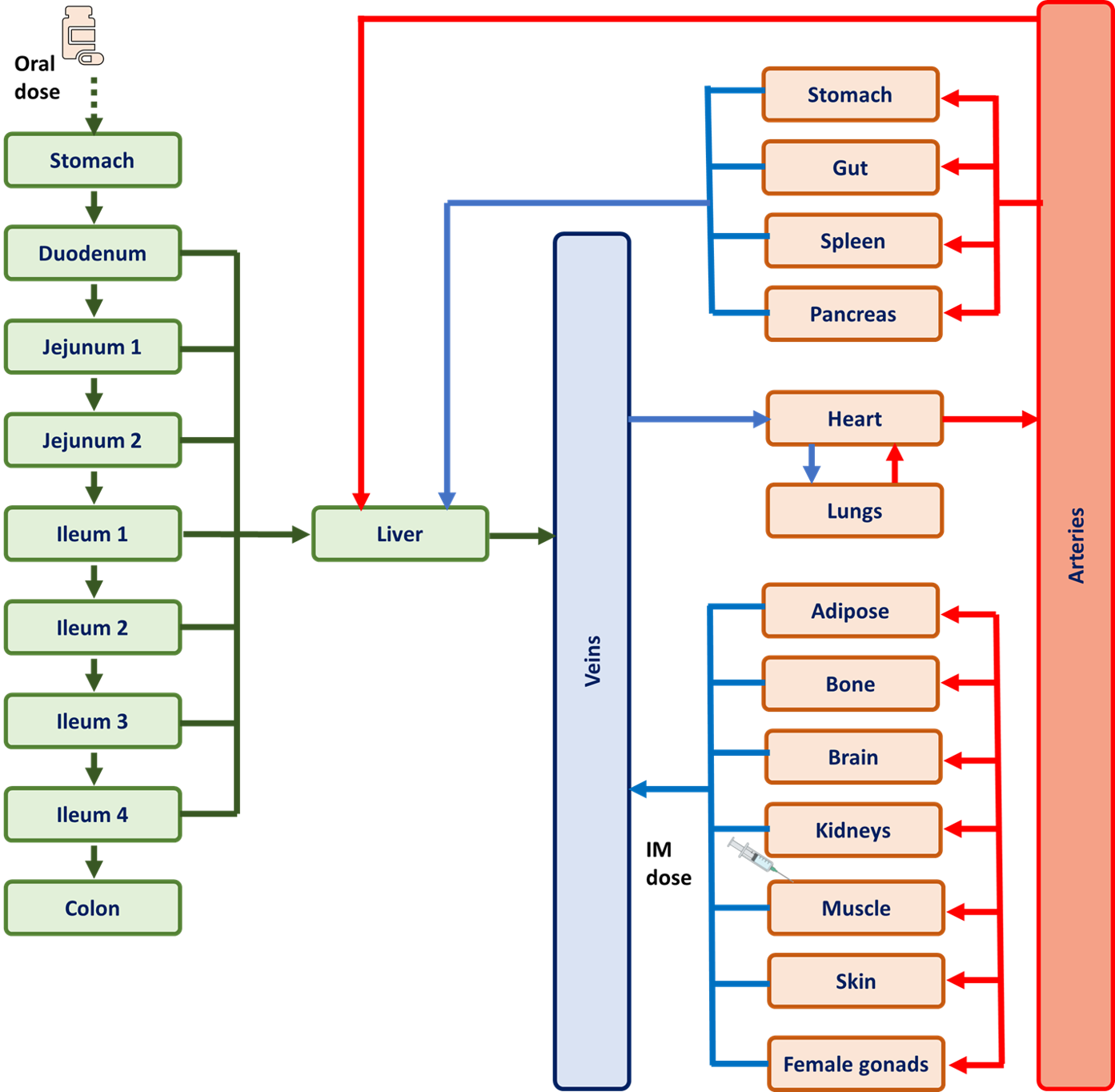
Aim Long-acting cabotegravir and rilpivirine have been approved to manage HIV in adults, but data regarding safe use in pregnancy are limited. Physiologically-based pharmacokinetic modelling (PBPK) can predict drug disposition in complex populations. Approved dosing regimens were simulated in pregnancy to explore if Ctrough was maintained above target concentrations (664 ng/ml and 50 ng/ml respectively). Methods An adult PBPK model was developed and validated using clinical data of cabotegravir and rilpivirine in non-pregnant adults. This was modified by incorporating pregnancy-induced metabolic and physiological changes. The pregnancy PBPK model was validated with data on oral rilpivirine and raltegravir (UGT1A1 probe substrate) in pregnancy. Acceptance criteria for both adult and pregnancy models was absolute average-fold error (AAFE) < 2 between clinical and simulated values. The pregnancy PBPK model was used to simulate 12 weeks’ disposition of monthly and bimonthly dosing of long-acting cabotegravir and rilpivirine, initiated at different trimesters. Results Models were successfully qualified with all AAFE values below 2. Predicted Ctrough at week 12 for both monthly and bimonthly long-acting cabotegravir was above 664 ng/ml throughout pregnancy. Similarly, predicted Ctrough at week 12 for monthly long-acting rilpivirine was above 50 ng/ml throughout pregnancy. However, for bimonthly rilpivirine administration, predicted Ctrough at week 12 were <50 ng/ml in 1, 0.5, and 2.3% of the pregnant population when initiated in first, second, and third trimester respectively. Conclusion Model predictions suggest monthly and bimonthly long-acting cabotegravir is likely to maintain antiviral efficacy throughout pregnancy. However, bimonthly long-acting rilpivirine requires careful clinical evaluation in pregnancy.