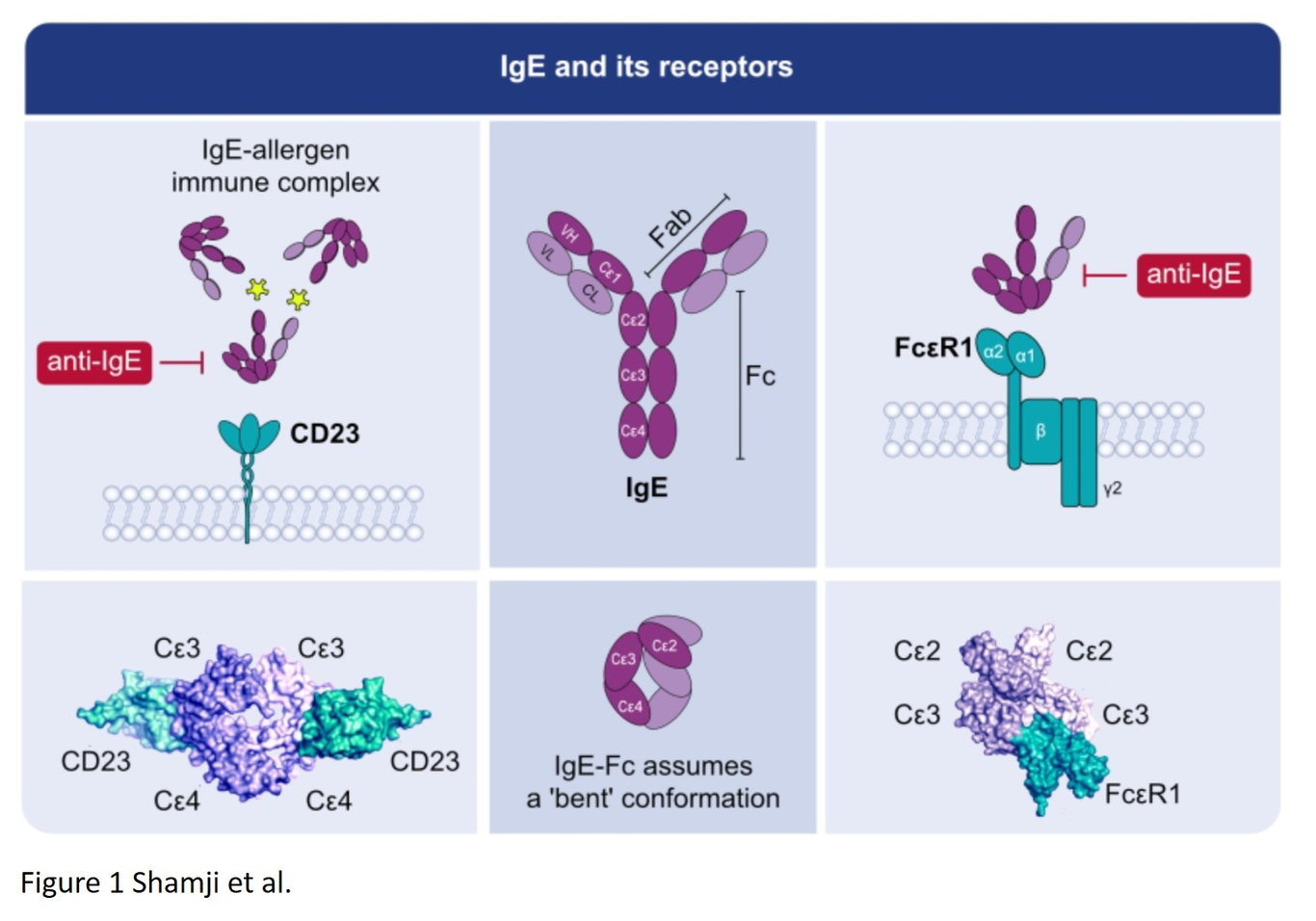
Immunoglobulin E (IgE)-mediated allergy is the most common hypersensitivity disease affecting more than 30% of the population. In genetically-predisposed subjects exposure to minute quantities of allergens leads to the production of IgE antibodies which is termed allergic sensitization and mainly occurs in early childhood. Allergen-specific IgE then binds to the high (FcRI) and low affinity receptors (FcRII, also called CD23) for IgE on effector cells and antigen-presenting cells, respectively. Subsequent and repeated allergen exposure increases allergen-specific IgE levels and, by receptor cross-linking, triggers immediate release of inflammatory mediators from mast cells and basophils whereas IgE-facilitated allergen presentation perpetuates T cell-mediated allergic inflammation. Due to engagement of receptors which are highly selective for IgE even tiny amounts of allergens can induce massive inflammation. Naturally occurring allergen-specific IgG and IgA antibodies usually recognize different epitopes on allergens compared to IgE, and do not efficiently interfere with allergen-induced inflammation. However IgG and IgA antibodies to these important IgE epitopes can be induced by allergen-specific immunotherapy or by passive immunization. These will lead to competition with IgE for binding with the allergen and prevent allergic responses. Similarly, anti-IgE treatment does the same by preventing IgE from binding to its receptor on mastcells and basophils. Here we review the complex interplay of allergen-specific IgE, IgG and IgA and the corresponding cell receptors in allergic diseases and its relevance for diagnosis, treatment and prevention of allergy.