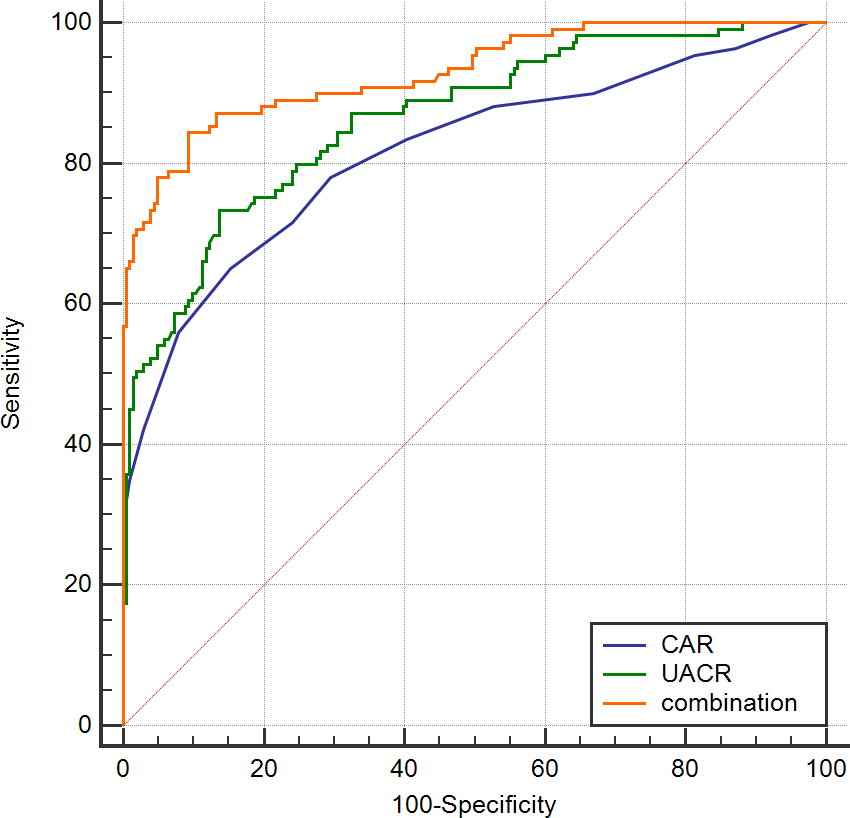
Aim: To evaluate the prognostic utility of C-reactive protein-albumin ratio (CAR) and urine protein-creatinine ratio (UACR) in patients with heart failure with preserved ejection fraction (HFpEF). Patients & methods: This study is a retrospective analysis. Patients diagnosed with HFpEF at the Jiangmen Central Hospital from January 2017 to January 2020 were included. HFpEF patients were stratified into two groups based on the occurrence of major adverse cardiac events (MACE). Receiver operator characteristic (ROC) curves were then constructed and Cox regression models were employed to gauge the prognostic relevance of CAR and UACR for HFpEF patients. Kaplan-Meier analysis evaluated the survival and MACE-free rate in patients with different level of CAR and UACR. Results: A total of 312 patients with HFpEF were enrolled in this study and followed up for 25.18±7.54 months. Among them, 109 MACE (34.94%), 59 all-cause mortality (18.91%). The age, level of C reactive protein (CRP), albumin (ALB), creatinine (Cr) , B-type pro-brain natriuretic peptide (NT-ProBNP) , CAR and UACR were statistically different between the MACE group and Non-MACE group ( P<0.05). Multivariate analysis showed that CAR and UACR were independent predictors of all-cause mortality and MACE in HFpEF patients. ROC showed that the AUC of the combination predicting the occurrence of all-cause mortality and MACE are 0.837 and 0.929 respectively. Kaplan-Meier analysis showed that the survival rate of group 1 (CAR≦0.16 and UACR≦29.15mg/g) was significantly higher than that of group 2 (CAR>0.16 or UACR>29.15mg/g) and group 3 (CAR>0.16 and UACR>29.15mg/g) (98.57% vs. 74.77 vs. 53.85%, P=0.000) and MACE-free survival rate of group 1 (CAR≦0.16 and UACR≦31.05mg/g) was significantly higher than that of group 2 ( CAR>0.16 or UACR>31.05mg/g) and group 3 (CAR>0.16 and UACR>31.05mg/g) (94.37% vs. 48.35 vs. 13.11%, P=0.000). Conclusion: We determined that increased CAR and UACR was independently associated with poor outcomes in HFpEF patients. Combined evaluation of CAR and UACR yielded a more accurate predictive model of HFpEF patient outcomes relative to the use of either of these metrics in isolation. Our research can provide a theoretical basis in the occurrence of MACE for the high-risk HFpEF patients and intervene them properly and timely.