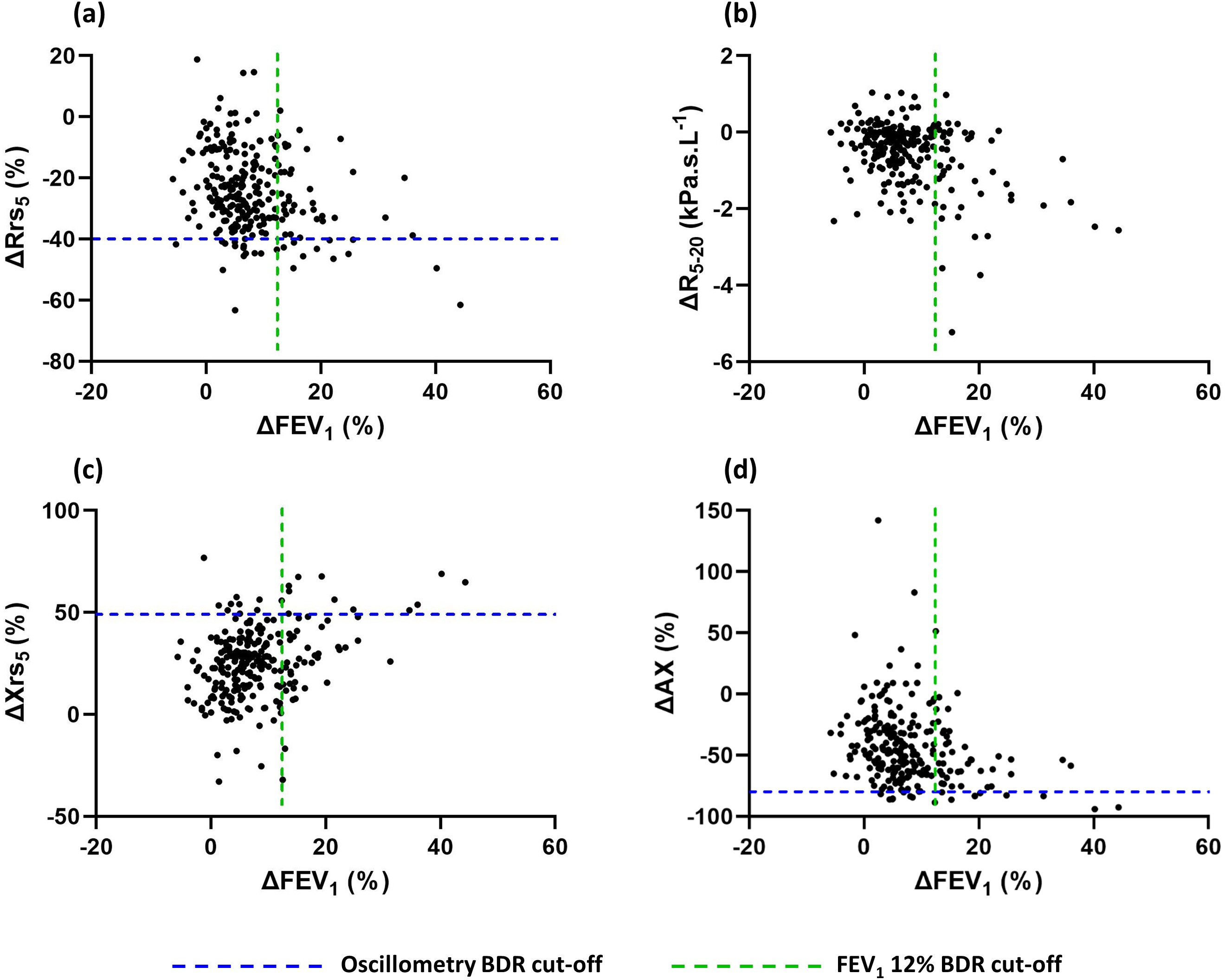
Introduction: The European Respiratory Society Oscillometry Taskforce identified that clinical correlates of bronchodilator responses are needed to advance oscillometry in clinical practice. The understanding of bronchodilator-induced oscillometry changes in preterm lung disease is poor. Here we describe a comparison of bronchodilator assessments performed using oscillometry and spirometry in a population born very preterm and explore the relationship between bronchodilator-induced changes in respiratory function and clinical outcomes. Methods: Participants aged 6-23 born ≤32 (N=288; 132 with bronchopulmonary dysplasia) and ≥37 weeks’ gestation (N=76, term-born controls) performed spirometry and oscillometry. A significant bronchodilator response (BDR) to 400mcg salbutamol was classified according to published criteria. Results: A BDR was identified in 30.9% (n=85) of preterm-born individuals via spirometry and/or oscillometry, with poor agreement between spirometry and oscillometry definitions (k=0.26; 95%CI 0.18 to 0.40, p<0.001). Those born preterm with a BDR by oscillometry but not spirometry had increased wheeze (33% vs 11%, p=0.010) and baseline resistance (Rrs 5 z-score mean difference (MD)= 0.86, 95%CI 0.07 to 1.65, p=0.025), but similar spirometry to the group without a BDR (FEV 1 z-score MD= -0.01, 95%CI -0.66 to 0.68, p>0.999). Oscillometry was more feasible than spirometry (95% vs 85% (FEV 1), 69% (FVC), p<0.001), however being born preterm did not affect test feasibility. Conclusion: In the preterm population, oscillometry is a feasible and clinically useful supportive test to assess the airway response to inhaled salbutamol. Changes measured by oscillometry reflect related but distinct physiological changes to that measured by spirometry and thus these tests should not be used interchangeably.