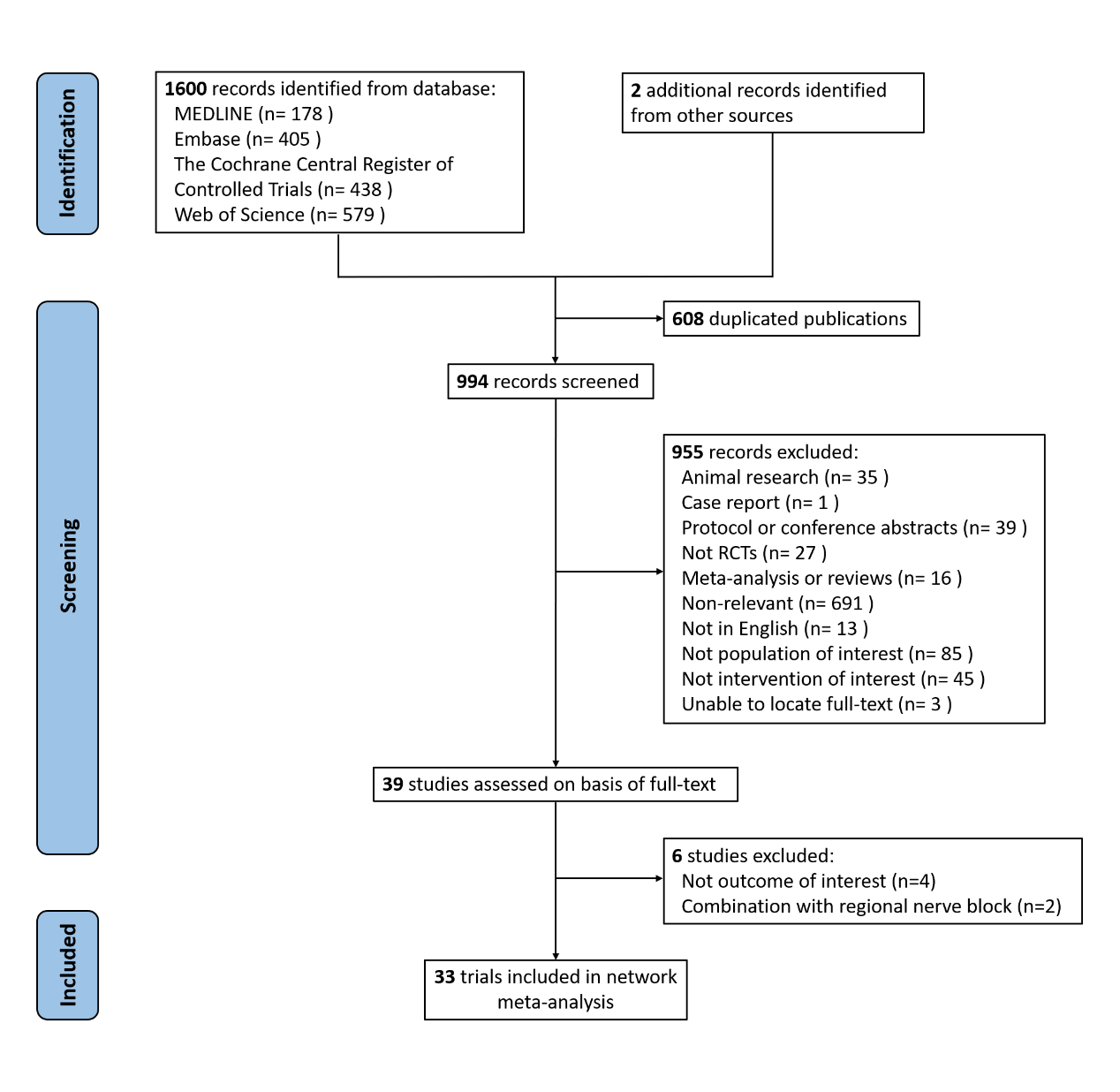
Background: Opioid-induced hyperalgesia (OIH) is an adverse event after exposure to opioids which would increase pain intensity. The optimal drug to prevent these adverse effects is still unclear. We aimed to perform a network meta-analysis to compare different pharmacological interventions in preventing the increase in postoperative pain caused by OIH. Methods: Several databases were searched independently for randomized-controlled trials (RCTs) comparing different pharmacological interventions in preventing OIH. The primary outcomes were postoperative pain intensity at rest at 24h and the incidence of postoperative nausea and vomiting (PONV). Secondary outcomes included pain thresholds at 24h after surgery, cumulative morphine consumption over 24h, time to first postoperative analgesic requirement, and the incidence of shivering. Results: In all, 33 RCTs comprising 1711 patients were identified. In terms of postoperative pain intensity, amantadine, magnesium sulphate, pregabalin, dexmedetomidine, ibuprofen, flurbiprofen plus dexmedetomidine, parecoxib, parecoxib plus dexmedetomidine, and S (+)-ketamine plus methadone were associated with milder pain intensity than placebo, with amantadine ranked the most effective (SUCRA values =96.2). In terms of the incidence of PONV, intervene with dexmedetomidine or flurbiprofen plus dexmedetomidine means a lower incidence placebo and dexmedetomidine showed the best result (SUCRA values =90.3). Conclusions: Amantadine was identified as the best in postoperative pain intensity as well as non-inferior to placebo in the incidence of PONV. Dexmedetomidine was the only intervention that is superior to placebo in all indicators.