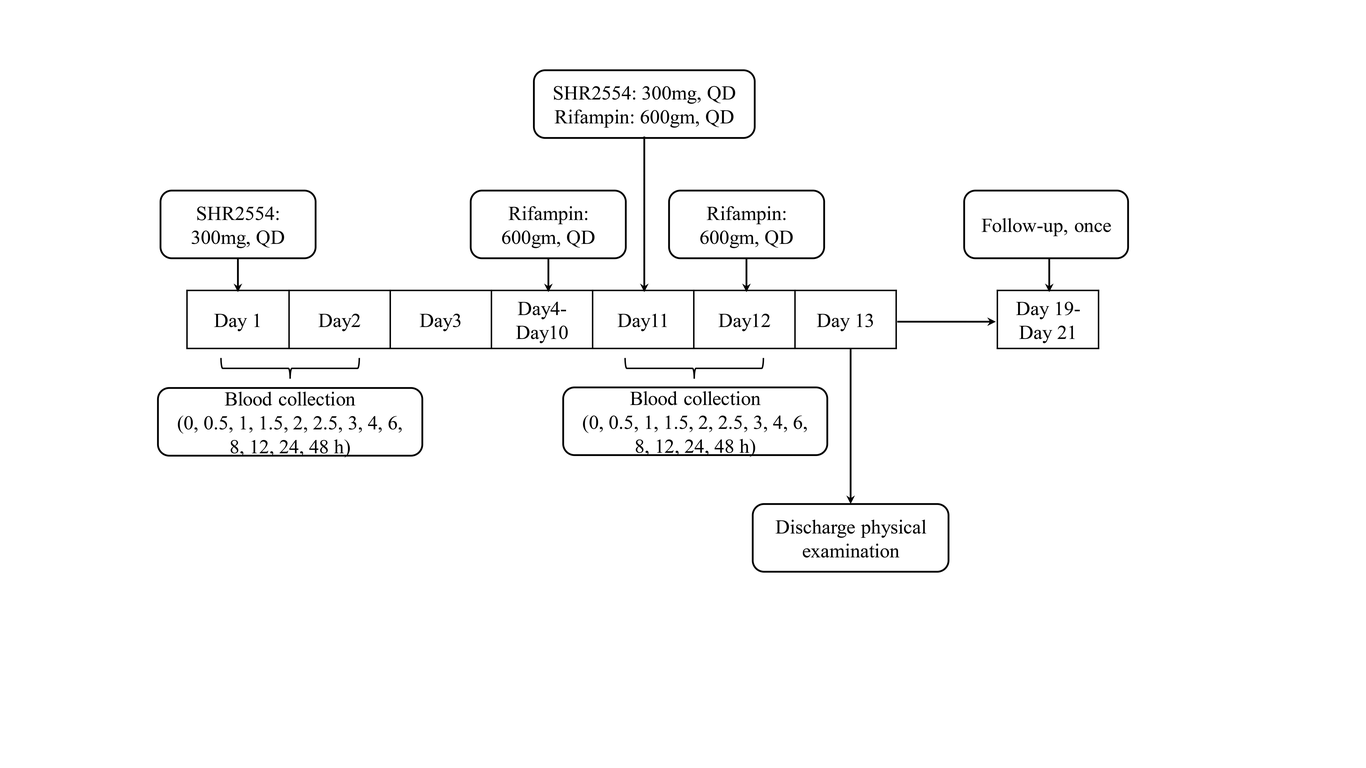
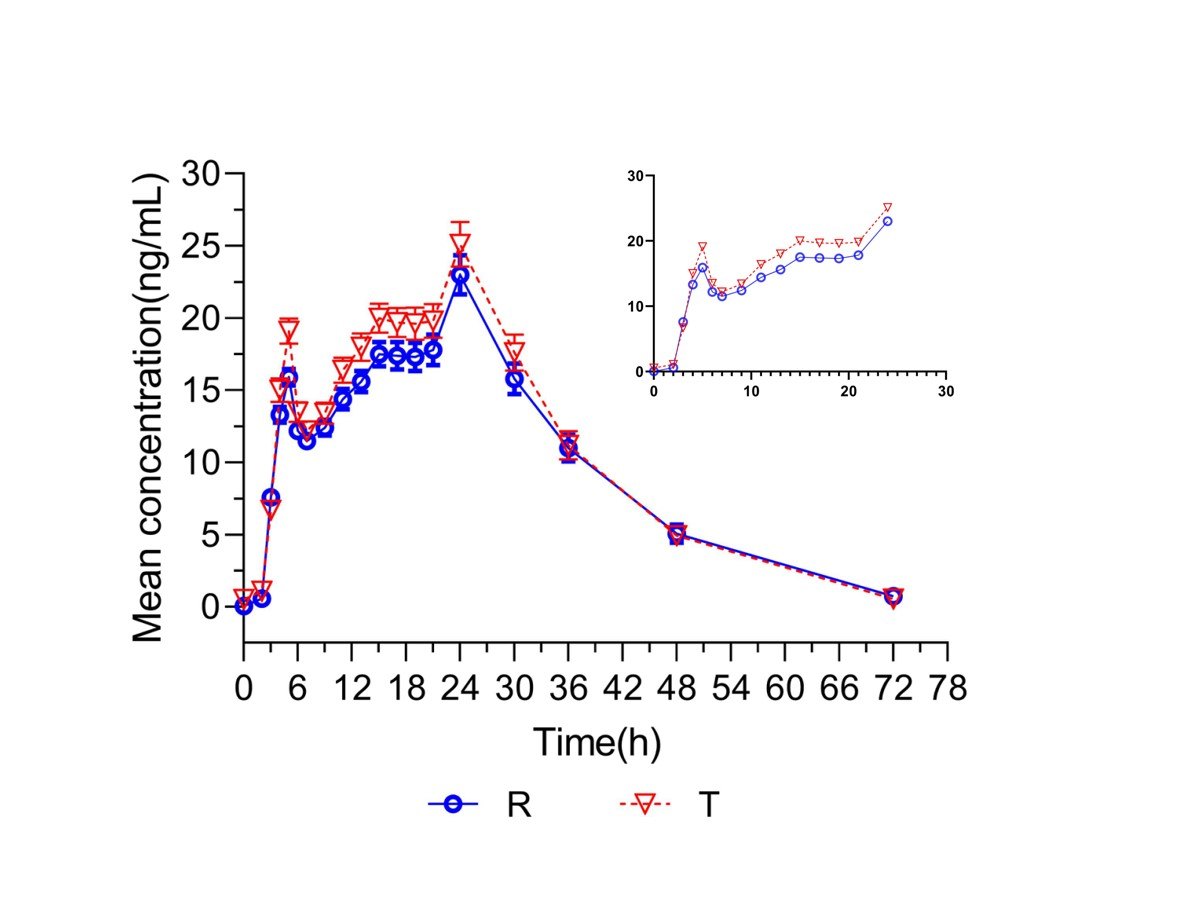
Aims: A phase I open-label study assessed the effect of multiple oral doses of a potent CYP3A4 inducer (rifampicin) on the pharmacokinetic profile of SHR2554, a novel enhancer of zeste homolog 2 inhibitor (EZH2) and CYP3A4 substrate. Methods: Eighteen adult Chinese healthy subjects were enrolled in this study. All participants received a single oral dose of SHR2554 (300 mg) on day 1, rifampin (600 mg) from day 4 to day 10 and day 12, the same dose was coadministered with SHR2554 (300 mg) and rifampicin (600 mg) on day 11. The primary endpoints were SHR2554 exposure parameters. Lack of drug–drug interaction was concluded if 90% confidence intervals (CIs) for the ratio of area under the plasma concentration–time curve (AUC) or maximum concentration (Cmax), with/without oral rifampicin, were within a pre-specified interval (0.80–1.25). Results: The Cmax, AUC0-t, and AUC0-∞ of administration alone and coadministration with rifampin were 177.265 ±127.9889 ng/mL, 17.001 ± 8.4759 ng/mL; 672.12 ± 507.390 h*ng/mL, 38.58 ± 19.495 h*ng/mL; and 721.50 ±514.386 h*ng/mL, 46.30 ± 20.750 h*ng/mL, respectively. Coadministration with rifampin decreased the least-squares geometric mean ratios of Cmax, AUC0-t, and AUC0-∞ by 89%, 93%, and 93%, respectively. Well tolerance and acceptable safety profile showed during the trial. Conclusion: The exposure of SHR2554 was significantly decreased when coadministered with rifampicin. It is recommended to avoid concomitant use of SHR2554 and strong inducers of CYP3A4.