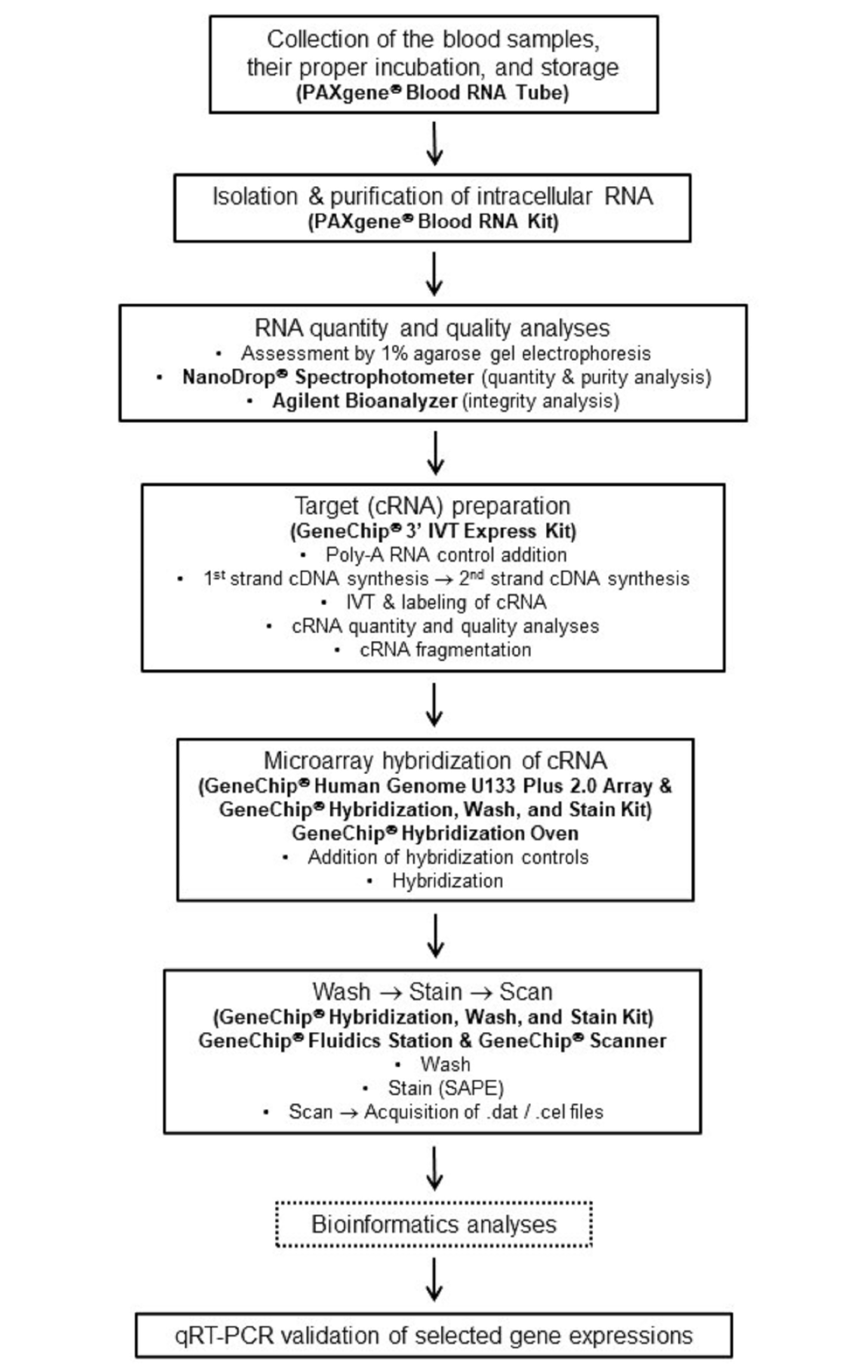
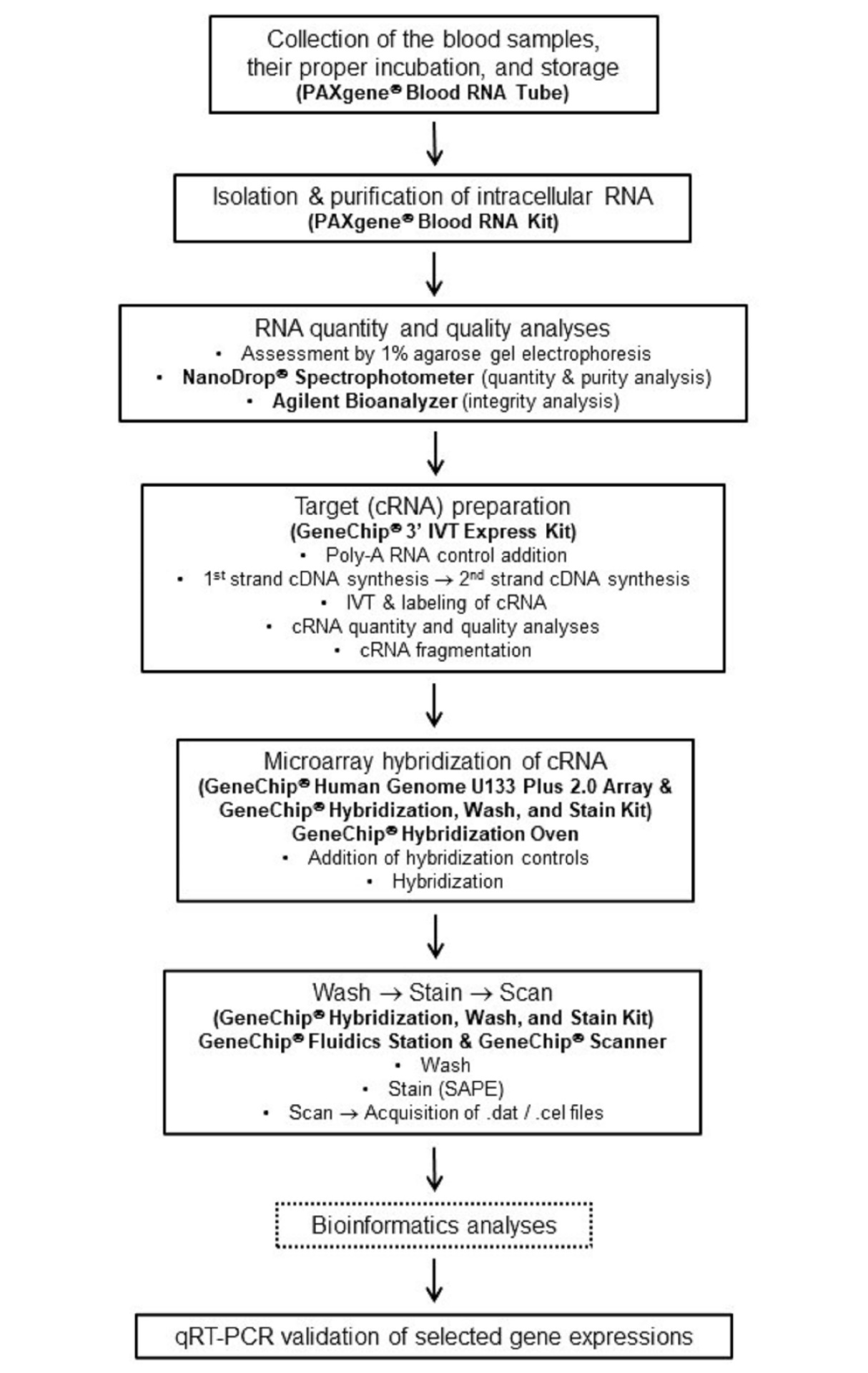
AbstractBehçet syndrome (BS) is a chronic, multisystemic inflammatory condition with unanswered questions regarding its pathogenesis and rational therapeutics. A microarray-based comparative transcriptomic analysis was performed to elucidate the molecular mechanisms of BS and identify any potential therapeutic targets. Twenty-nine BS patients (B) and 15 age and sex-matched control subjects (C) were recruited. Patients were grouped as mucocutaneous (M), ocular (O), and vascular (V) according to their clinical phenotypes. GeneChip Human Genome U133 Plus 2.0 arrays were used for expression profiling on peripheral blood samples of the patients and the control subjects. Following documentation of the differentially expressed gene (DEG) sets, the data were further evaluated with bioinformatics analysis, visualization, and enrichment tools. Validation of the microarray data was performed using qRT-PCR. When P <0.05 and fold change >2.0 were chosen, the following numbers of DEGs were obtained; B vs. C: 28, M vs. C: 20, O vs. C: 8, V vs. C: 555, M vs. O: 6, M vs. V: 324, O vs. V: 142. Venn diagram analysis indicated only two genes, CLEC12A and IFI27, in the intersection of M vs. C and O vs. C and V vs. C. Another noteworthy gene appeared as CLC in the DEG sets. Cluster analyses successfully clustered distinct clinical phenotypes of BS. While innate immunity-related processes were enriched in the M group, adaptive immunity-specific processes were significantly enriched in the O and V groups. Distinct clinical phenotypes of BS patients displayed distinct expression profiles. In Turkish BS patients, expression differences regarding the genes CLEC12A, IFI27, and CLC seemed to be operative in the disease pathogenesis. Based on these findings, future research should consider the immunogenetic heterogeneity of BS clinical phenotypes. Two anti-inflammatory genes, namely CLEC12A and CLC, may be valuable as therapeutic targets and may also help design an experimental model in BS.IntroductionBehçet syndrome (BS) is a chronic, multisystemic inflammatory condition characterized by a relapsing and remitting course.1Initially defined by Dr. Hulusi Behçet as a “triple symptom complex” including oral and genital ulcers and uveitis, BS may present with diverse mucocutaneous, ocular, musculoskeletal, gastrointestinal, pulmonary, cardiovascular, and central nervous system manifestations, which are primarily vasculitic in origin.2,3Even though more than eight decades have passed since its definition, there are essential questions regarding BS that still need to be answered. The etiopathogenesis of the condition and its rational therapeutics are among these questions waiting for an answer. Three important properties of BS, namely (1) the divergent and sometimes paradoxical immunological findings observed in the studies, (2) the occurrence of diverse clinical features among different ethnic groups, and (3) the distinct clinical phenotype clusters within the syndrome, complicate the clarification of a sound, shared, and comprehensive etiopathogenesis for BS.4,5 Elucidating the disease mechanisms of BS at the molecular level may enable the scientific community to find the answers to the questions mentioned above, including the pathogenesis of BS, and may help develop novel, effective, and safer treatment approaches for the syndrome.Previously, by borrowing the microarray data (Gene Expression Omnibus [GEO] data repository, GEO accession GSE17114) of the study by Xavier et al.6, our group has demonstrated the presence of significant differences in gene expression and disease pathways between mucocutaneous, ocular, and vascular BS groups in a Portuguese BS patient population.5 Additionally, in the same study, four functional gene groups, namely (1) negative regulators of inflammation (CD69 , CLEC12A ,TNFAIP3 ), (2) neutrophil granule proteins (LTF ,OLFM4 , AZU1 , MMP8 , DEFA4 , CAMP ), (3) antigen processing and presentation proteins (CTSS ,ERAP1 ), and (4) regulators of immune response (LGALS2 ,BCL10 , ITCH , CEACAM8 , CD36 , IL8 ,CCL4 , EREG , NFKBIZ , CCR2 , CD180 ,KLRC4 , NFAT5 ) were shown to be potentially instrumental in BS immunopathogenesis.5In our present study, we performed a microarray-based comparative genome-wide expression analysis in Turkish BS patients and a sex and age-matched healthy control group. We aimed (1) to elucidate the molecular disease mechanisms in Turkish BS patients, (2) to document any discrepancies between BS clinical phenotypes/patient subgroups regarding these disease mechanisms, and (3) to identify any potential therapeutic targets for BS.