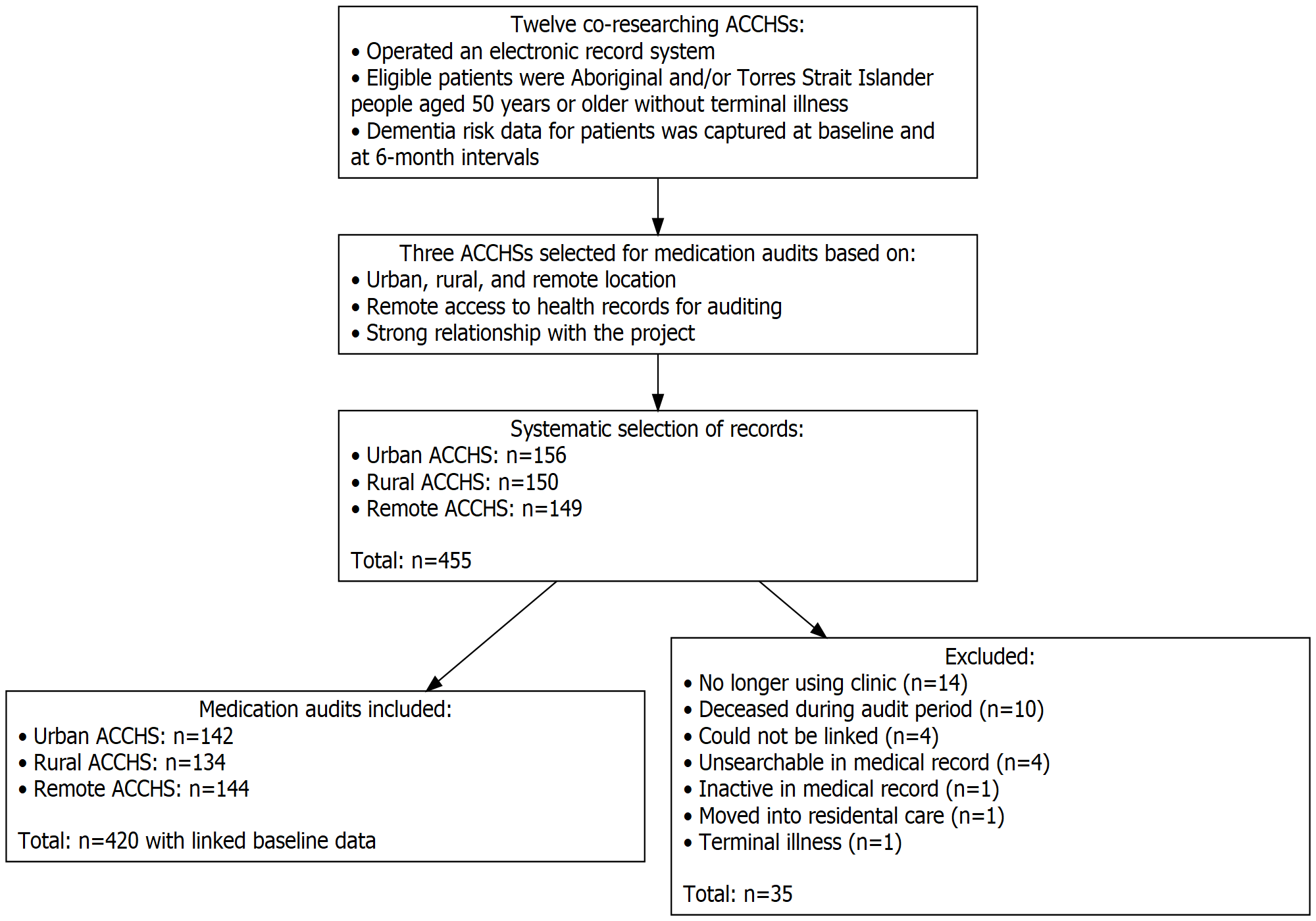
Aim Prevalence of potentially suboptimal prescribing and associated risk factors were investigated among older patients attending primary care via Aboriginal Community Controlled Health Services (ACCHSs). Methods Prescription medications were audited for 420 systematically selected patients aged ≥50 years at three ACCHSs in urban, rural, and remote settings. Polypharmacy, potentially inappropriate medications (PIMs), and anticholinergic burden (ACB) were estimated and associated risk factors explored with logistic regression. Results The prevalence of polypharmacy, use of PIMs, and ACB score ≥3, was 43%, 18%, and 12%, respectively. In multivariable logistic regression analyses, polypharmacy was less likely in rural (OR=0.43, 95% CI=0.24-0.77) compared to urban health service patients, and more likely in those with heart disease (OR=2.62, 95% CI=1.62-4.25), atrial fibrillation (OR=4.25, 95% CI=1.08-16.81), hypertension (OR=2.14, 95% CI=1.34-3.44), diabetes (OR=2.72, 95% CI=1.69-4.39), or depression (OR=1.91, 95% CI=1.19-3.06). PIMs were more frequent in females (OR=1.88, 95% CI=1.03-3.42), and less frequent in rural (OR=0.41, 95% CI=0.19-0.85) and remote (OR=0.58, 95% CI=0.29-1.18) patients. Factors associated with PIMs were kidney disease (OR=2.60, 95% CI=1.37-4.92), urinary incontinence (OR=3.00, 95% CI=1.02-8.83), depression (OR=2.67, 95% CI=1.50-4.77), heavy alcohol use (OR=2.83, 95% CI 1.39-5.75) and subjective cognitive concerns (OR=2.69, 95% CI=1.31-5.52). High anticholinergic burden was less common in rural (OR=0.10, 95% CI 0.03-0.34) and remote (OR=0.51, 95% CI 0.25-1.04) patients, and more common in those with kidney disease (OR=3.07, 95% CI 1.50-6.30), or depression (OR=3.32, 95% CI 1.70-6.47). Conclusion Associations between potentially suboptimal prescribing and depression or cognitive concerns highlights the importance of considered medication review and deprescribing for these patients.