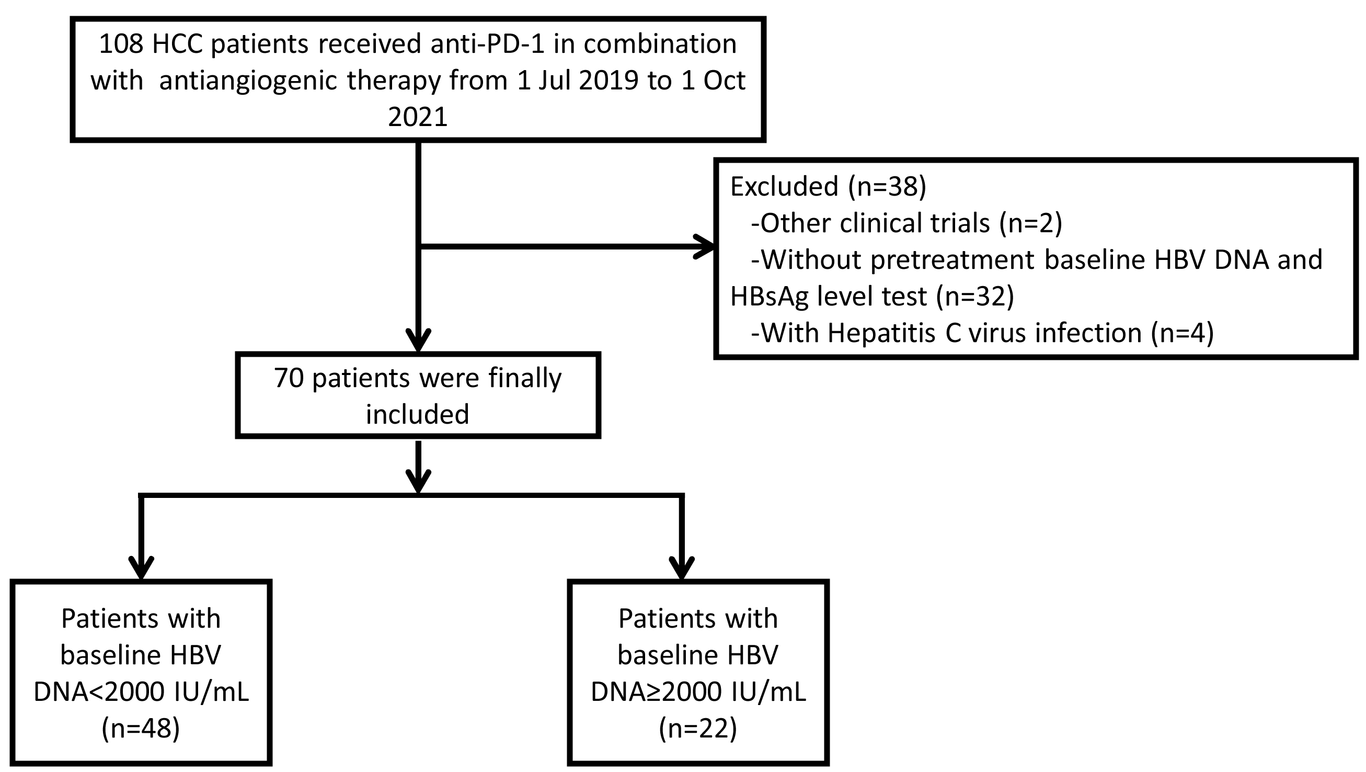
Aims: A high baseline hepatitis B virus (HBV) load has always been listed as an exclusion criterion for programmed cell death-1 (PD-1) inhibitor-associated therapy in clinical trials, as the interaction between HBV load and anti-PD-1/PD-L1 therapy remains controversial. Methods: We performed a retrospective cohort study of unresectable HCC patients who were seropositive for HBsAg and accepted tenofovir alafenamide fumarate (TAF) therapy before anti-PD-1 in combination with an antiangiogenic treatment. Patients were divided into a low HBV DNA group (≤ 2000 IU/ml) and a high HBV DNA group (> 2000 IU/ml) according to the baseline HBV DNA levels. Tumour response and progression-free survival (PFS) were compared, and univariate and multivariate Cox analyses were performed to identify potential risk factors for PFS. The incidences of HBV reactivation and HBV-associated hepatitis were also recorded. Results: Seventy eligible patients were included: 48 in the low group and 22 in the high group. The objective response rates (ORRs), disease control rates (DCRs), and PFS did not differ significantly between the two groups (P = 0.761, 0.552, and 0.784, respectively). The results of Cox analyses revealed that the baseline HBV load did not affect PFS. Additionally, HBV reactivation occurred in only 2 patients (2.9%), and no patient experienced HBV-related hepatic impairment when given a continuous TAF treatment. Conclusions: Baseline HBV loads do not affect the prognosis of HCC patients receiving anti-PD-1 in combination with an antiangiogenic therapy, while PD-1 inhibitors do not aggravate HBV reactivation and hepatic impairment in patients simultaneously subjected to TAF prophylaxis.